
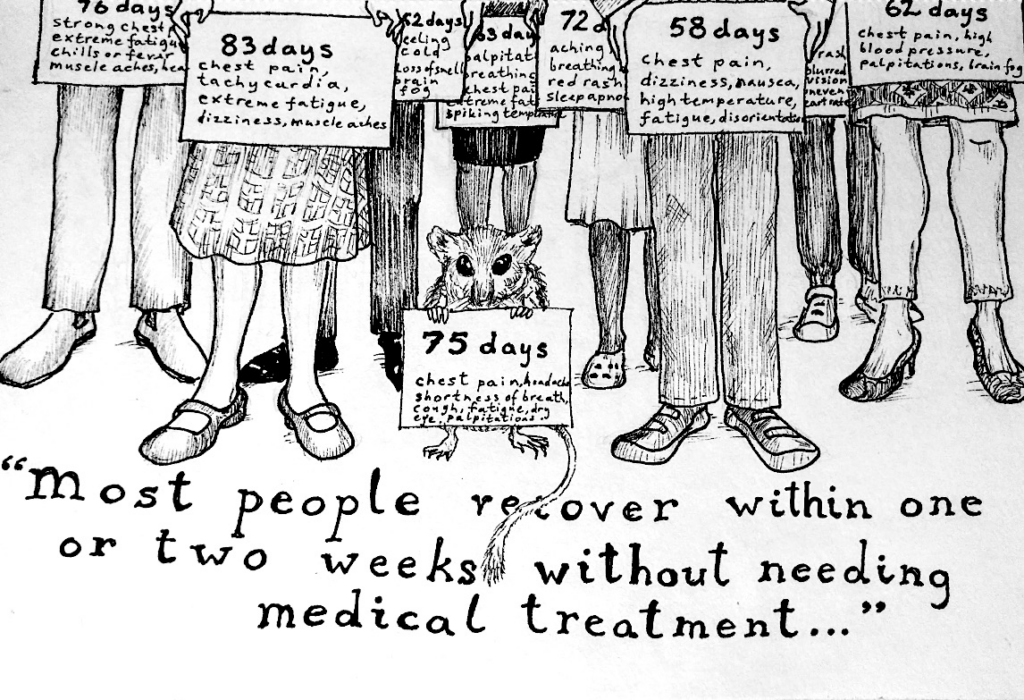
On Taking Long COVID Seriously
There was a time when doctors and patients inhabited a nearly “silent world,” as famously described by physician-educator Jay Katz in his 1984 book of the same name. In those days, communication ran in only one direction and trust was expected only in the other. Doctors explained things and patients listened quietly, to be followed by grateful compliance. Fortunately, medical schools have emphasized mutual communication and things have gotten much better. Doctors and patients now work together, forming a relationship in which the patient’s input is sought and experiences valued. But not always. Physicians’ receptivity turns out to have its limits, perhaps never more so than when patients organize around a demand for greater recognition.
Consider, for example, a recent New Yorker article by Dr. Dhruv Khullar, a faculty member at Weill Cornell Medical College, titled “The Struggle to Define Long COVID.” After allowing briefly that there is “little doubt among researchers that long COVID exists,” Khullar devotes much of the balance of the 6,000-word essay to his own considerable doubts about various patients’ conditions, especially those involved in patient-advocacy groups.
The problem with too many long COVID patients, according to Khullar, is that they do not appreciate medical skepticism. Rather than accept that their symptoms may be “psychologically generated,” as has often been urged by otherwise baffled treating physicians, they insist instead that the “syndrome be seen mainly as a physiological disease.” After all, says Khullar, “mental illness is still illness.” The balky patients are thus “setting rules about what kind of suffering counts.”
Khullar’s view borders perilously on a return to the silent world, in which patients are discouraged from objecting to possible misdiagnoses. The default to a psychological explanation – when all tests are negative – has profound problems of its own. First, it implicitly assumes that every possible physiological condition can already be identified by currently available tests. Moreover, biomedical research can be delayed or inhibited once a novel syndrome is labeled primarily psychogenic. Finally, psychiatry itself has a poor historical record, having too often claimed physical diseases – including multiple sclerosis, asthma, and peptic ulcers – as psychosomatic or conversion disorders.
In any case, Khullar’s skepticism strangely vanishes when it comes to a group of long COVID denying physicians. He uncritically quotes Dr. Jeremy Devine, a young Canadian psychiatrist still in his residency, who implausibly asserts that long COVID – a worldwide phenomenon affecting hundreds of thousands or more – is “largely an invention of vocal patient activist groups.” Many diseases have at first been poorly understood, but it does not follow that they must then be deemed psychogenic.
“America has often seemed divided between two tribes,” observes Khullar, “one that ignores scientists and another that listens to them.” The long COVID advocates, he explains, belong in a third category of “people who take every precaution and yet stand in broad opposition to the scientific establishment.”
Khullar could not be more wrong. Far from opposing the medical establishment, long COVID survivors are trying desperately to get its attention. Yes, some patients are prone to exaggeration and even hyperbole, including certain leaders of the advocacy movement; others may unthinkingly blame long COVID for unrelated symptoms. But Khullar’s disproportionate focus on extreme stories – such as a patient who attributed tooth loss to long COVID – is unhelpful and misleading. The great majority of patients understand full well that objective medical research – not of the ivermectin sort – is essential to address their illness. They quite reasonably fear, however, that their experiences will be discounted and their voices ignored.
Worrying that the survivors’ movement has failed to “embrace a rational approach to its suffering,” Khullar offers his assurance that “clinicians and researchers [have] devoted their careers, however imperfectly, to helping patients.” The challenge for patients is therefore to trust their doctors and suspend their obstinate misgivings. “Dogma obscures data,” he says, and “when skepticism becomes taboo, progress grows more difficult.” If medical dogma itself has ever obstructed progress – note: it has – Khullar does not mention it.
Responding to criticism on Twitter, Khullar explained that his goal had been “to describe the challenges of diagnosing a new medical condition—not to cast doubt on whether it exists.” That will come as good news to many readers, including those who were dismayed by his patronizing reference to “people who say they suffer from chronic-fatigue syndrome,” a condition actually recognized as a “serious, chronic, complex, and multisystem disease” in a 2015 report by the U.S. Institute of Medicine.
Today’s doctors are formally taught, as Khullar puts it, that patients should have a “stronger presence . . . as authentic partners in the project of improving the human condition.” Those are noble sentiments, but they tend to give way in practice. Faced with uncertain symptoms and no clear precedents, it is understandably difficult for doctors to credit what their patients are telling them. It is so much easier to refer them to psychiatrists.
I do not doubt the benevolence of physicians like Dhruv Khullar, who sincerely wish that patients would be satisfied by their good intentions. But condescension in the name of compassion is no way to build trust.
Steven Lubet, JD, was diagnosed with chronic fatigue syndrome (ME/CFS) in 2006.


















































































This is good, but I need to point out that attributing tooth loss to Long Covid isn’t an extreme story. Sufferers have been reporting this for over a year and several articles have been written about it. Although it hasn’t been formally studied, it’s hypothesized that it could be a result of vascular damage. I first heard of it when someone’s dentist said they’d seen a lot of post-Covid patients with brew dental problems.